Pes Planus?
Overview

Feet are very variable in shape within and between ethnic groups as well as in populations generally. There is not a normal profile but a wide variation with people with foot profiles at the extremes being very high arched or very low arched, with most people somewhere nearer the middle. What will dictate the general profile of a foot is the bony shape and the soft tissue support. The first thing to say about flat feet and fallen arches is that they are not medical terms and therefore have different meaning to different people. Therefore this question is not as easy as it first might seem. Pes Planus is the medical term for flat feet.
Causes
There are several reasons why arches fall. It can be genetic, it can be a result of unsupported shoes, a product of our lives and the pressure we put on the feet. Some people have active lifestyles so the wear and tear effect on the muscles there that runs down the back of the calf and wraps around the arch can slacken as we get older. It can be a number of things.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms below. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered.
pes planus radiology
Non Surgical Treatment
During walking and running, there is a small natural inward drop (slight pronation) that is part of the spring and propulsion. Allowing exaggerated sagging is like rounding your shoulders too much. Legs and feet have posture that you can control yourself. Use your own muscles and get free built-in exercise and arch support all day, and stop painful poor positioning. Some people with existing abnormality or growths in the ball of the foot will roll inward (or outward) to get the pressure off the deformed area because standing straight hurts. See your doctor first. Remember, don't force. If it hurts, it's wrong. All you are doing is learning how to stand neutral, not tilted so much that you compress the joints. The concept is to hold your feet in the same healthful position that shoe supports would. It is like an ice skater holds their skates straight at the ankle, not angled.
Surgical Treatment

Feet that do not respond to the treatments above may need surgery. The surgery will help to create a supportive arch.
Feet are very variable in shape within and between ethnic groups as well as in populations generally. There is not a normal profile but a wide variation with people with foot profiles at the extremes being very high arched or very low arched, with most people somewhere nearer the middle. What will dictate the general profile of a foot is the bony shape and the soft tissue support. The first thing to say about flat feet and fallen arches is that they are not medical terms and therefore have different meaning to different people. Therefore this question is not as easy as it first might seem. Pes Planus is the medical term for flat feet.
Causes
There are several reasons why arches fall. It can be genetic, it can be a result of unsupported shoes, a product of our lives and the pressure we put on the feet. Some people have active lifestyles so the wear and tear effect on the muscles there that runs down the back of the calf and wraps around the arch can slacken as we get older. It can be a number of things.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms below. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
You can always give yourself the ?wet test? described above to see whether you have flat feet. Most people who do not notice their flat feet or have no pain associated with them do not think to see a foot doctor. Flat feet can lead to additional problems such as stiffness or pain, however, especially if the condition appears out of nowhere. If you think you may have flat feet, you should seek medical attention to ensure there are no additional issues to worry about. Your doctor will be able to diagnose you with a number of tests. For example, he or she may have you walk around, stand still, or stand on your tiptoes while you are being examined. Your doctor may also examine your foot?s shape and functionality. It?s important to let your foot doctor know about your medical and family history. In some cases, your doctor may order imaging tests such as x-rays or an MRI (magnetic resonance imaging) to determine a cause of your flat foot. If tarsal coalition is suspected in children, a CT scan is often ordered.
pes planus radiology
Non Surgical Treatment
During walking and running, there is a small natural inward drop (slight pronation) that is part of the spring and propulsion. Allowing exaggerated sagging is like rounding your shoulders too much. Legs and feet have posture that you can control yourself. Use your own muscles and get free built-in exercise and arch support all day, and stop painful poor positioning. Some people with existing abnormality or growths in the ball of the foot will roll inward (or outward) to get the pressure off the deformed area because standing straight hurts. See your doctor first. Remember, don't force. If it hurts, it's wrong. All you are doing is learning how to stand neutral, not tilted so much that you compress the joints. The concept is to hold your feet in the same healthful position that shoe supports would. It is like an ice skater holds their skates straight at the ankle, not angled.
Surgical Treatment
Feet that do not respond to the treatments above may need surgery. The surgery will help to create a supportive arch.
Heel Lifts For Leg Length Discrepancy After Hip Replacement
Overview
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Causes
From an anatomical stand point, the LLD could have been from hereditary, broken bones, diseases and joint replacements. Functional LLD can be from over pronating, knee deformities, tight calves and hamstrings, weak IT band, curvature in the spine and many other such muscular/skeletal issues.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).

how can a man look taller?
Surgical Treatment
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Causes
From an anatomical stand point, the LLD could have been from hereditary, broken bones, diseases and joint replacements. Functional LLD can be from over pronating, knee deformities, tight calves and hamstrings, weak IT band, curvature in the spine and many other such muscular/skeletal issues.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The most accurate method to identify leg (limb) length inequality (discrepancy) is through radiography. It?s also the best way to differentiate an anatomical from a functional limb length inequality. Radiography, A single exposure of the standing subject, imaging the entire lower extremity. Limitations are an inherent inaccuracy in patients with hip or knee flexion contracture and the technique is subject to a magnification error. Computed Tomography (CT-scan), It has no greater accuracy compared to the standard radiography. The increased cost for CT-scan may not be justified, unless a contracture of the knee or hip has been identified or radiation exposure must be minimized. However, radiography has to be performed by a specialist, takes more time and is costly. It should only be used when accuracy is critical. Therefore two general clinical methods were developed for assessing LLI. Direct methods involve measuring limb length with a tape measure between 2 defined points, in stand. Two common points are the anterior iliac spine and the medial malleolus or the anterior inferior iliac spine and lateral malleolus. Be careful, however, because there is a great deal of criticism and debate surrounds the accuracy of tape measure methods. If you choose for this method, keep following topics and possible errors in mind. Always use the mean of at least 2 or 3 measures. If possible, compare measures between 2 or more clinicians. Iliac asymmetries may mask or accentuate a limb length inequality. Unilateral deviations in the long axis of the lower limb (eg. Genu varum,?) may mask or accentuate a limb length inequality. Asymmetrical position of the umbilicus. Joint contractures. Indirect methods. Palpation of bony landmarks, most commonly the iliac crests or anterior iliac spines, in stand. These methods consist in detecting if bony landmarks are at (horizontal) level or if limb length inequality is present. Palpation and visual estimation of the iliac crest (or SIAS) in combination with the use of blocks or book pages of known thickness under the shorter limb to adjust the level of the iliac crests (or SIAS) appears to be the best (most accurate and precise) clinical method to asses limb inequality. You should keep in mind that asymmetric pelvic rotations in planes other than the frontal plane may be associated with limb length inequality. A review of the literature suggest, therefore, that the greater trochanter major and as many pelvic landmarks should be palpated and compared (left trochanter with right trochanter) when the block correction method is used.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, which vary among osteopaths, physiotherapist and chiropractor and whether the LLD is functional or structural. Thus is a combination of myofascial release (massage) & stretching of shortened muscles. Manipulation or mobilization of the spine, sacro-iliac joint (SIJ), hip, knee, foot. Orthotics, shoe lifts can be used to treat discrepancies from two to six cm (usually up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear). Surgery (epiphysiodesis, epiphyseal stapling,bone resection).
how can a man look taller?
Surgical Treatment
Many people undergo surgery for various reasons - arthritis, knee replacement, hip replacement, even back surgery. However, the underlying cause of leg length inequality still remains. So after expensive and painful surgery, follow by time-consuming and painful rehab, the true culprit still remains. Resuming normal activities only continues to place undue stress on the already overloaded side. Sadly so, years down the road more surgeries are recommended for other joints that now endure the excessive forces.
All You Should Understand About
Overview
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term).
Causes
A flattening or overstretching of your plantar fascia can cause microscopic tears, inflammation, and a burning sensation. While developing slowly, there may be a sudden severe event sometimes occurring in only one foot at a time. Plantar Faciitis can affect people of all ages and backgrounds. Some contributing factors include age, weight-bearing activities, sudden increase in physical activity, improper shoes, excess weight or a recent weight gain (as little as 5 pounds), and poor biomechanics (flat feet, high arches or unnatural gait).
Symptoms
Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
Essentially rest from aggravating activity, physiotherapy treatment to alleviate the inflammatory component, stretching the tight calf, strengthening up of the intrinsic muscles of the foot e.g. tissue scrunch, picking up pens etc. and correction of biomechanical problems in the foot e.g. orthotics. Sometimes, a heel cup or pad to relieve pressure - a donut type pad may be helpful. Strapping has been shown to be helpful, especially in circumstances where the patient can?t wear orthotics - the foot is strapped to help support the arch. There has been limited success with cortisone injections or surgery and the latter is very rarely required.
Surgical Treatment
It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation.
how to add a strap to high heels
Prevention

Being overweight can place excess pressure and strain on your feet, particularly on your heels. Losing weight, and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet, can be beneficial for your feet. Wearing appropriate footwear is also important. Ideally, you should wear shoes with a low to moderate heel that supports and cushions your arches and heels. Avoid wearing shoes with no heels.
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term).
Causes
A flattening or overstretching of your plantar fascia can cause microscopic tears, inflammation, and a burning sensation. While developing slowly, there may be a sudden severe event sometimes occurring in only one foot at a time. Plantar Faciitis can affect people of all ages and backgrounds. Some contributing factors include age, weight-bearing activities, sudden increase in physical activity, improper shoes, excess weight or a recent weight gain (as little as 5 pounds), and poor biomechanics (flat feet, high arches or unnatural gait).
Symptoms
Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day.
Diagnosis
A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem.
Non Surgical Treatment
Essentially rest from aggravating activity, physiotherapy treatment to alleviate the inflammatory component, stretching the tight calf, strengthening up of the intrinsic muscles of the foot e.g. tissue scrunch, picking up pens etc. and correction of biomechanical problems in the foot e.g. orthotics. Sometimes, a heel cup or pad to relieve pressure - a donut type pad may be helpful. Strapping has been shown to be helpful, especially in circumstances where the patient can?t wear orthotics - the foot is strapped to help support the arch. There has been limited success with cortisone injections or surgery and the latter is very rarely required.
Surgical Treatment
It is rare to need an operation for heel pain. It would only be offered if all simpler treatments have failed and, in particular, you are a reasonable weight for your height and the stresses on your heel cannot be improved by modifying your activities or footwear. The aim of an operation is to release part of the plantar fascia from the heel bone and reduce the tension in it. Many surgeons would also explore and free the small nerves on the inner side of your heel as these are sometimes trapped by bands of tight tissue. This sort of surgery can be done through a cut about 3cm long on the inner side of your heel. Recently there has been a lot of interest in doing the operation by keyhole surgery, but this has not yet been proven to be effective and safe. Most people who have an operation are better afterwards, but it can take months to get the benefit of the operation and the wound can take a while to heal fully. Tingling or numbness on the side of the heel may occur after operation.
how to add a strap to high heels
Prevention
Being overweight can place excess pressure and strain on your feet, particularly on your heels. Losing weight, and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet, can be beneficial for your feet. Wearing appropriate footwear is also important. Ideally, you should wear shoes with a low to moderate heel that supports and cushions your arches and heels. Avoid wearing shoes with no heels.
Mortons Neuroma An Overview
Overview
 Morton's neuroma is a painful foot condition that occurs when a nerve, usually between the third and fourth toes, expands and becomes compressed. Shoes, particularly high heels or shoes with tight toe boxes, and walking often make the pain worse. In some cases, patients with Morton's neuroma find short-term pain relief when they do not put weight on the affected foot.
Morton's neuroma is a painful foot condition that occurs when a nerve, usually between the third and fourth toes, expands and becomes compressed. Shoes, particularly high heels or shoes with tight toe boxes, and walking often make the pain worse. In some cases, patients with Morton's neuroma find short-term pain relief when they do not put weight on the affected foot.
Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Patients will complain of numbness, a ?pins and needles? type of tingling and loss of sensation in the toes. Burning pain in the ball of the foot that may radiate into the toes. The pain generally intensifies with activity or wearing shoes. Night pain is rare. There may also be numbness in the toes, or an unpleasant feeling in the toes. Runners may feel pain as they push off from the starting block. High-heeled shoes, which put the foot in a similar position to the push-off, can also aggravate the condition. Tight, narrow shoes also aggravate this condition by compressing the toe bones and pinching the nerve.
Diagnosis
A doctor can usually identify Morton's neuroma during a physical exam. He or she will squeeze or press on the bottom of your foot or squeeze your toes together to see if it hurts. Your doctor may also order an X-ray of your foot to make sure nothing else is causing the pain.
Non Surgical Treatment
Rest. Continuing with normal training will increase pain and inflammation and prevent the injury from healing. Wear a metatarsal pad under the forefoot which will raise and spread the bones of the forefoot taking the pressure off the nerve. Wearing metatarsal pads in the shoes under the forefoot spreads the metatarsals creating more space for the nerve. See a sports injury professional who can advise on treatment and rehabilitation. Orthotic inserts may be required to correct any biomechanical dysfunction of the foot.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
Morton's neuroma is a painful foot condition that occurs when a nerve, usually between the third and fourth toes, expands and becomes compressed. Shoes, particularly high heels or shoes with tight toe boxes, and walking often make the pain worse. In some cases, patients with Morton's neuroma find short-term pain relief when they do not put weight on the affected foot.Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Patients will complain of numbness, a ?pins and needles? type of tingling and loss of sensation in the toes. Burning pain in the ball of the foot that may radiate into the toes. The pain generally intensifies with activity or wearing shoes. Night pain is rare. There may also be numbness in the toes, or an unpleasant feeling in the toes. Runners may feel pain as they push off from the starting block. High-heeled shoes, which put the foot in a similar position to the push-off, can also aggravate the condition. Tight, narrow shoes also aggravate this condition by compressing the toe bones and pinching the nerve.
Diagnosis
A doctor can usually identify Morton's neuroma during a physical exam. He or she will squeeze or press on the bottom of your foot or squeeze your toes together to see if it hurts. Your doctor may also order an X-ray of your foot to make sure nothing else is causing the pain.
Non Surgical Treatment
Rest. Continuing with normal training will increase pain and inflammation and prevent the injury from healing. Wear a metatarsal pad under the forefoot which will raise and spread the bones of the forefoot taking the pressure off the nerve. Wearing metatarsal pads in the shoes under the forefoot spreads the metatarsals creating more space for the nerve. See a sports injury professional who can advise on treatment and rehabilitation. Orthotic inserts may be required to correct any biomechanical dysfunction of the foot.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
Shoe Lifts The Answer To Leg Length Difference
There are actually two different kinds of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is anatomically shorter than the other. As a result of developmental periods of aging, the brain senses the gait pattern and identifies some variance. The entire body usually adapts by tilting one shoulder over to the "short" side. A difference of less than a quarter inch is not really abnormal, require Shoe Lifts to compensate and typically does not have a profound effect over a lifetime.

Leg length inequality goes typically undiscovered on a daily basis, yet this issue is simply remedied, and can reduce quite a few instances of upper back pain.
Therapy for leg length inequality typically involves Shoe Lifts. Most are very reasonably priced, ordinarily priced at below twenty dollars, in comparison to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Back ache is easily the most widespread ailment afflicting men and women today. Around 80 million people have problems with back pain at some point in their life. It is a problem that costs businesses huge amounts of money each year on account of time lost and production. New and superior treatment methods are constantly sought after in the hope of reducing the economical influence this issue causes.

People from all corners of the world suffer the pain of foot ache due to leg length discrepancy. In these situations Shoe Lifts might be of worthwhile. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic orthopedists.
So that you can support the body in a nicely balanced fashion, feet have a very important part to play. Despite that, it is sometimes the most overlooked area in the human body. Some people have flat-feet meaning there is unequal force placed on the feet. This causes other body parts including knees, ankles and backs to be impacted too. Shoe Lifts make sure that correct posture and balance are restored.
Leg length inequality goes typically undiscovered on a daily basis, yet this issue is simply remedied, and can reduce quite a few instances of upper back pain.
Therapy for leg length inequality typically involves Shoe Lifts. Most are very reasonably priced, ordinarily priced at below twenty dollars, in comparison to a custom orthotic of $200 or higher. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Back ache is easily the most widespread ailment afflicting men and women today. Around 80 million people have problems with back pain at some point in their life. It is a problem that costs businesses huge amounts of money each year on account of time lost and production. New and superior treatment methods are constantly sought after in the hope of reducing the economical influence this issue causes.
People from all corners of the world suffer the pain of foot ache due to leg length discrepancy. In these situations Shoe Lifts might be of worthwhile. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic orthopedists.
So that you can support the body in a nicely balanced fashion, feet have a very important part to play. Despite that, it is sometimes the most overlooked area in the human body. Some people have flat-feet meaning there is unequal force placed on the feet. This causes other body parts including knees, ankles and backs to be impacted too. Shoe Lifts make sure that correct posture and balance are restored.
What Is The Most Suitable Strategy For Calcaneal Spur

Overview
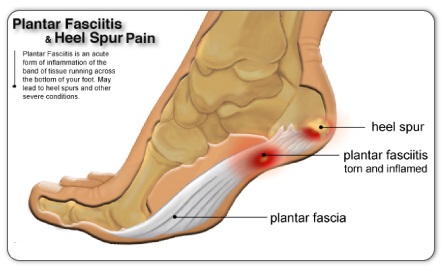
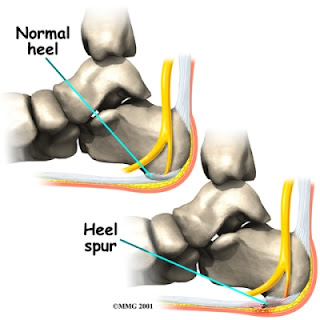
A heel spur is a calcium deposit causing a bony protrusion on the underside of the heel bone. On an X-ray, a heel spur can extend forward by as much as a half-inch. Without visible X-ray evidence, the condition is sometimes known as "heel spur syndrome." Although heel spurs are often painless, they can cause heel pain. They are frequently associated with plantar fasciitis, a painful inflammation of the fibrous band of connective tissue (plantar fascia) that runs along the bottom of the foot and connects the heel bone to the ball of the foot. Treatments for heel spurs and associated conditions include exercise, custom-made orthotics, anti-inflammatory medications, and cortisone injections. If conservative treatments fail, surgery may be necessary.
Causes
There exists a membrane that covers most of the bone along the heel. When this membrane gets torn repeatedly due to straining of the muscles in the foot, the calcium deposits that lead to heel spurs are more likely to occur.

Symptoms
Heel spurs often do not show any symptoms. If you have intermittent or chronic pain when you walk, run or jog, it may be heel spur. There will be inflammation the point where spur formation happens. The pain is caused by soft tissue injury in the heel. Patients often describe the pain as a pin or knife sticking to the heel. The pain is more specially in the morning when the patient stands up for the first time.
Diagnosis
The proper diagnosis of a heel spur often requires an X-ray. To make this process as convenient for his patients as possible, most clinics have an on-site digital X-ray and diagnostic ultrasound machines. This can make it unnecessary for patients to visit diagnostic imaging centers, allowing patients to receive more expedient treatment.
Non Surgical Treatment
Ice and use arch support . If you can localize the spur, cut a hole in a pad of felt and lay the hole over the spur. This supports the area around the spur and reduces pressure on it. Massage the spur. Start gently with your thumb and gradually increase the pressure until you?re pushing hard directly on the spur with your knuckle or another firm object. Even it if hurts, it should help. Arch support. Build up an arch support system in your shoes. Try to equalize the pressure of your body weight throughout your arch and away from the plantar area. Use a ?cobra pad? or other device that supports the arch but releases pressure on the painful area. If homemade supports do not work, see a podiatrist about custom orthotics.
Surgical Treatment
Though conservative treatments for heel spurs work most of the time, there are some cases where we need to take your treatment to the next level. Luckily, with today?s technologies, you can still often avoid surgery. Some of the advanced technologies to treat a Heel Spur are Platelet Rich Plasma Therapy. Platelet Rich Plasma Therapy (also known as PRP) is one of several regenerative medicine techniques that University Foot and Ankle Institute has helped bring to foot and ankle care. This amazing in-office procedure allows the growth factors in the blood to be used to actually begin the healing process again long after your body has given up on healing the area. Heel Pain Shockwave Therapy. Shockwave therapy is a non-invasive procedure done in the office that allows for new blood to get to the region of fascia damage and help with healing. Results have been excellent with more than 70 percent of patients getting relief with only one treatment. Topaz for Heal Spurs and pain. Another minimally invasive technology technique is called Coblation Surgery using a Topaz probe. This minimally invasive procedure involves controlled heating of multiple tiny needles that are inserted through the skin and into the plantar fascia. This process, like PRP and Shockwave therapy, irritates the fascia enough to turn a chronic problem back into an acute problem, greatly increasing the chances of healing. Heel Spur Surgery. Endoscopic Plantar Fasciotomy is one surgical procedure that we consider to release the tight fascia. University Foot and Ankle Institute has perfected an endoscopic (camera guided) approach for fascia release to allow rapid healing and limited downtime with minimal pain.
Prevention
In 2002, researchers attempted to compare the effects of various running techniques on pronation and resulting injuries like stress fractures and heel spurs. They suggested that it is possible to teach runners to stride in such a way as to minimize impact forces. One way is to lower running speed. Another is to take longer rest periods following a run.
Inferior Calcaneal Spur Symtoms

Overview
A heel spur is a hooked bony growth protruding from the calcaneus or heel bone. It often occurs alongside plantar fasciitis, and as such the two conditions are often confused, however they are not the same.
Causes
Fctors that increase the risk of developing heel spurs include a high body mass index (BMI), regular vigorous activity, and intensive training routines or sports. Factors such as these are believed to increase the incidence of repetitive stress injuries that are associated with the formation of heel spurs. When a heel spur forms, extremely sharp pain along with the feeling that a part of the heel is trying to burst through the skin usually occurs. If left untreated, an individual may eventually begin to struggle to perform simple activities such as walking.
Symptoms
Heel spurs may or may not cause symptoms. Symptoms are usually related to the plantar fasciitis. You may experience significant pain. Your heel pain may be worse in the morning when you first wake up or during certain activities.
Diagnosis
Your doctor, when diagnosing and treating this condition will need an x-ray and sometimes a gait analysis to ascertain the exact cause of this condition. If you have pain in the bottom of your foot and you do not have diabetes or a vascular problem, some of the over-the-counter anti-inflammatory products such as Advil or Ibuprofin are helpful in eradicating the pain. Pain creams, such as Neuro-eze, BioFreeze & Boswella Cream can help to relieve pain and help increase circulation.
Non Surgical Treatment
Some heel spurs do require surgery, however surgery is a last resort. In most cases the patients underlying foot problem needs to be addressed, such as Over Pronation and Over Supination and Heel Pain Treatment Options need to be implemented if Plantar Fasciitis and Achilles Tendonitis are still an ongoing concern. Your best treatment is always prevention.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.